We deploy our proprietary Generative Phosphoproteomics AP3 (Acrivon Predictive Precision Proteomics) platform for rational drug design and predictive clinical development. Our clinical pipeline currently includes two potentially first-in-class programs targeting the pathways involved in DNA Damage Response (DDR) and cell cycle regulation. We are also advancing an additional AP3-driven preclinical cell cycle program in IND-enabling studies.


Acrivon Pipeline
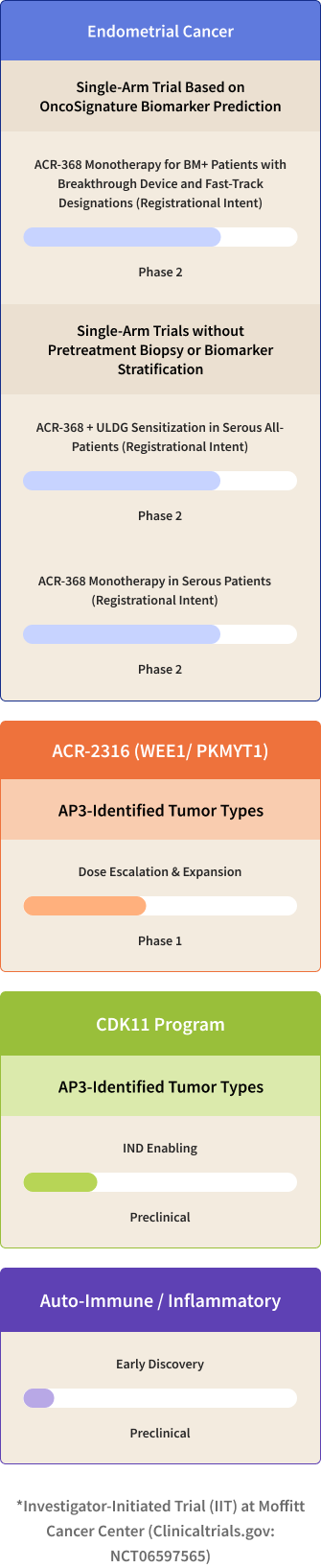
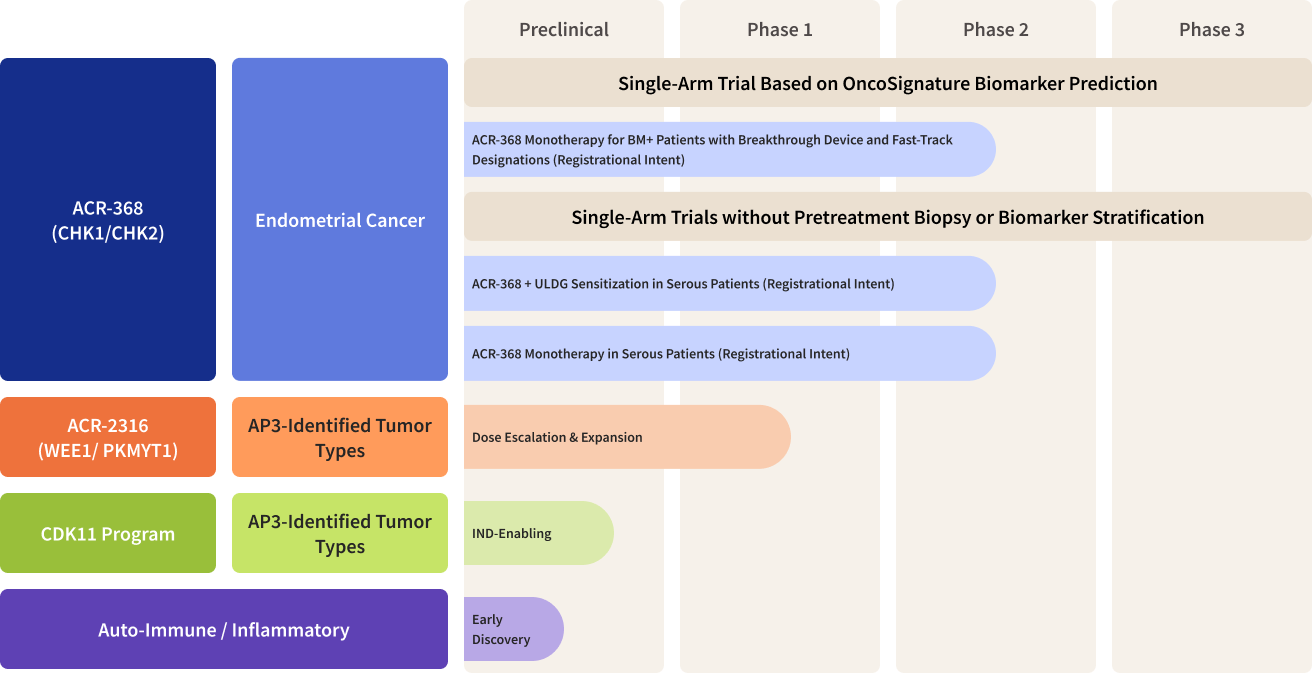
Acrivon’s Lead Program ACR-368 (also known as Prexasertib, in-licensed from Lilly), is a clinically-advanced, potent selective inhibitor of the DNA Damage Response checkpoint kinases, CHK1 and CHK2. ACR-368 has demonstrated deep, durable single-agent anti-tumor clinical activity, including complete responses, in a proportion of patients with platinum-resistant ovarian cancer* and squamous cell cancer ‡. Using OncoSignature, we have identified endometrial cancer as a high unmet need solid tumor type predicted to be highly sensitive to the drug candidate. The company has received fast track designation from the Food and Drug Administration, or FDA, for the investigation of ACR-368 as monotherapy based on OncoSignature-predicted sensitivity in patients with endometrial cancer or platinum-resistant ovarian cancer. The FDA has granted Breakthrough Device designations for the ACR-368 OncoSignature assay for the identification of patients with endometrial cancer or for patients with ovarian cancer, who may benefit from ACR-368 treatment. Acrivon is also leveraging its proprietary AP3 precision medicine platform for developing its co-crystallography-driven, internally developed pipeline programs, consisting of its clinical candidate, ACR-2316, a selective, dual WEE1/PKMYT1 inhibitor and ACR-6840, a development candidate (along with several other equally promising candidates) targeting CDK11. More information on our clinical trials can be found on clinicaltrials.gov, and information on our Expanded Access Policy can be found here.
*Ref: Lee et al, Lancet Oncology (2018); Konstantinopoulos et al, Gynec Onc (2022); ‡ Ref: Hong et al, CCR (2018)